Flu 2026–2027: What the New WHO Vaccine Update Means for You (and Why It Matters Now)
Flu season may still be lingering in some countries, but global health experts are already looking ahead. On 27 February 2026, the World Health Organization released its official recommendations for the 2026–2027 Northern Hemisphere influenza vaccine composition.
That might sound routine. It isn’t.
Every year, scientists must predict which influenza viruses will dominate months in advance. Vaccine manufacturers then need time to produce millions of doses before flu season typically begins in October. When the match is strong, vaccines significantly reduce hospitalizations and deaths. When the virus evolves unexpectedly, the stakes rise.
Here’s what changed for 2026–2027 — and what it means for you.
Why Flu Vaccines Change Every Year
Influenza viruses are shape-shifters.
They mutate constantly, especially in two key surface proteins:
-
Hemagglutinin (H)
-
Neuraminidase (N)
These proteins are what your immune system recognizes. When they change enough, last year’s antibodies may not fully recognize this year’s virus. That’s why the flu shot isn’t “one and done.”
To stay ahead, the WHO convenes experts from its Global Influenza Surveillance and Response System (GISRS) — the world’s longest-running disease surveillance network (active since 1952). They analyze thousands of virus samples collected globally and decide which strains vaccine makers should target next.
It’s essentially global viral forecasting.
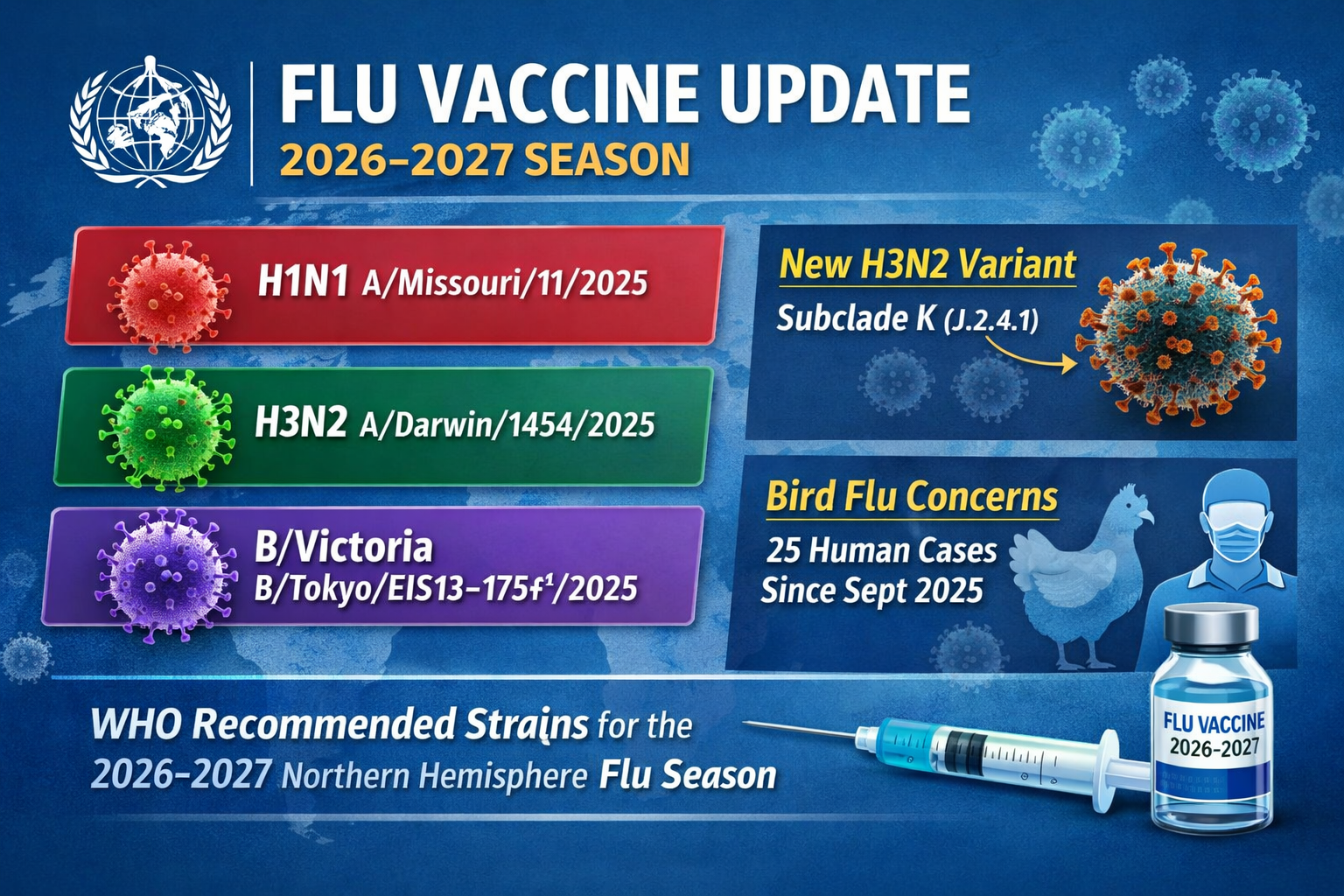
The 2026–2027 Recommended Flu Strains (Northern Hemisphere)
For the upcoming season, the WHO recommends protection against three main influenza groups:
Egg-Based Vaccines
-
A/Missouri/11/2025 (H1N1)pdm09-like virus
-
A/Darwin/1454/2025 (H3N2)-like virus
-
B/Tokyo/EIS13-175/2025 (B/Victoria lineage)-like virus
Cell-Based, Recombinant, or Nucleic Acid Vaccines
-
A/Missouri/11/2025 (H1N1)pdm09-like virus
-
A/Darwin/1415/2025 (H3N2)-like virus
-
B/Pennsylvania/14/2025 (B/Victoria lineage)-like virus
If you notice slight differences between egg-based and cell-based versions, that’s intentional.
Why Some Vaccine Strains Differ by Manufacturing Type
Most traditional flu vaccines are grown in eggs. But growing viruses in eggs can introduce small adaptive mutations — changes that help the virus grow in eggs but may slightly alter its structure compared to circulating human strains.
Cell-based and newer platform vaccines avoid some of these egg-adaptation changes. As a result, the WHO sometimes recommends slightly different “like” strains for different production technologies.
This is particularly important for H3N2, a subtype known for rapid mutation and for causing more severe seasons in older adults.
In short:
Different manufacturing platforms aim to improve how closely the vaccine matches the viruses actually spreading in communities.
The Big Story: A New H3N2 Variant Emerges
In August 2025, a noticeably different H3N2 variant began spreading globally. Classified as J.2.4.1 and informally known as “subclade K,” it quickly became dominant in multiple regions.
Why that matters:
-
It contributed to earlier flu season starts in several countries.
-
Some regions reported higher-than-usual activity.
-
H3N2 historically leads to more hospitalizations in older populations.
The 2026–2027 vaccine update reflects the need to address this rapidly spreading variant.
Viruses don’t wait politely for public health agencies to catch up. This is an attempt to stay ahead.
What About Influenza B?
The recommended vaccine includes protection against the B/Victoria lineage.
Notably absent? B/Yamagata lineage.
No confirmed B/Yamagata cases have been reported globally since March 2020. While scientists continue monitoring for its re-emergence, current surveillance supports focusing on B/Victoria.
This shift reflects real-world epidemiology, not guesswork.
Zoonotic Influenza: The “Bird Flu” Factor
Seasonal flu isn’t the only concern.
WHO experts also reviewed animal-origin influenza viruses that have infected humans. These zoonotic viruses can become dangerous if they gain the ability to spread easily between people.
Since late September 2025:
-
25 human infections
-
Across six countries
-
Mostly linked to exposure to infected animals or contaminated environments
-
No confirmed sustained human-to-human transmission
At the meeting, experts recommended developing a new candidate vaccine virus (CVV) for A(H9N2) — a bird flu strain.
Think of CVVs as emergency blueprints. If H9N2 begins spreading efficiently in humans, manufacturers could move faster to produce a pandemic vaccine.
Preparedness isn’t panic — it’s insurance.
How Serious Is Seasonal Influenza?
Globally, influenza causes:
-
Around 1 billion cases annually
-
3–5 million severe cases
-
Between 290,000 and 650,000 respiratory deaths each year
In the United States alone this season, flu has already caused:
-
At least 25 million illnesses
-
Around 20,000 deaths
-
Dozens of pediatric fatalities
Flu is not “just a bad cold.” It can lead to pneumonia, heart complications, worsening of chronic illnesses, and long hospital stays — particularly in vulnerable populations.
Does the Flu Shot Still Help If It’s Not a Perfect Match?
Yes.
Even in years where the match isn’t ideal, vaccines typically:
-
Reduce severe illness
-
Lower hospitalization rates
-
Decrease ICU admissions
-
Shorten illness duration
-
Reduce risk of death
Protection isn’t binary (all or nothing). It’s a spectrum.
A partially matched vaccine can still blunt the impact significantly.
Who Should Prioritize the 2026–2027 Flu Shot?
While annual vaccination is recommended for most people over six months old, it is especially important for:
-
Adults over 65
-
Pregnant individuals
-
Children under five
-
People with heart, lung, kidney, or metabolic disease
-
Immunocompromised individuals
-
Healthcare workers
-
Caregivers of high-risk individuals
Higher-dose or enhanced vaccines are often recommended for older adults to strengthen immune response.
The Future: Toward Faster and Broader Flu Vaccines
Scientists are working toward next-generation influenza vaccines that could:
-
Be manufactured faster (e.g., mRNA platforms)
-
Cover more strains
-
Offer longer-lasting immunity
-
Reduce reliance on annual reformulation
Researchers are also pursuing a so-called “universal” flu vaccine — one that targets stable parts of the virus that don’t mutate easily.
Several candidates are in clinical trials, though experts caution that fully universal protection remains scientifically challenging.
In the meantime, incremental improvements in strain selection, manufacturing speed, and vaccine potency continue to reduce seasonal risk.
What You Should Do Now
-
Plan: Flu shots are typically available in the early fall.
-
Don’t wait for peak season: Protection takes about two weeks to build.
-
Consider your risk profile: Age and medical conditions matter.
-
Stay informed: Local public health guidance may evolve if unusual patterns emerge.
Flu prevention isn’t just about personal protection. It also reduces strain on hospitals and protects vulnerable community members.
The Bottom Line
The 2026–2027 Northern Hemisphere flu vaccine recommendations reflect:
-
The emergence of a new H3N2 variant
-
Ongoing dominance of H1N1 and B/Victoria
-
Continued vigilance regarding zoonotic threats like H9N2
-
Refinement of strain selection across vaccine technologies
Influenza evolves constantly. Global surveillance and rapid updates are how public health stays one step ahead.
Flu season may feel routine, but the science behind it is anything but.
When vaccines become available later this year, getting immunized remains one of the most effective tools we have to reduce serious illness — both for yourself and your community.
References:
- https://www.bbc.com/future/article/20260227-why-is-there-no-universal-flu-vaccine
- https://www.scientificamerican.com/article/the-who-just-made-its-predictions-for-the-2026-2027-flu-season/
- https://www.who.int/news/item/27-02-2026-recommendations-for-influenza-vaccine-composition-for-the-2026-2027-northern-hemisphere-season